Wen-Jun Jiao,
Hua Li ![]() ,
Tian-Yi Li,
Tao Feng,
Su-Jun Li
,
Tian-Yi Li,
Tao Feng,
Su-Jun Li
For correspondence:- Hua Li Email: hualijwj@163.com
Received: 12 April 2016 Accepted: 10 September 2016 Published: 31 October 2016
Citation: Jiao W, Li H, Li T, Feng T, Li S. Effect of insulin pump infusion on comprehensive stress state of patients with diabetic ketoacidosis. Trop J Pharm Res 2016; 15(10):2283-2287 doi: 10.4314/tjpr.v15i10.30
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To assess changes in the comprehensive stress state of patients with diabetic ketoacidosis (DKA) following treatment with insulin infusion pump.
Methods: A total of 240 patients suffering from DKA who received treatment at The First Affiliated Hospital of Zhengzhou University from Feb. 2011 to Feb. 2014 were selected randomly and divided into a control group (120 cases), administered continuous intravenous insulin, and a treatment group (120 cases), administered insulin with an infusion pump. Relevant diabetes-associated serum indices, oxidative stress and stress hormone levels were compared between the groups at different time points.
Results: Levels of glycosylated haemoglobin (HbAlc), fasting blood glucose (FBG) and anion gap (AG) were lower (p < 0.05) in the treatment group than in the control group at various time points. Carbon dioxide combining power (CO2-CP) and C-reactive peptide levels in the treatment group were higher (p < 0.05) than those of the control group at different time points. Except for the level of methane dicarboxylic aldehyde (MDA), the values of other oxidative stress indices were higher (p < 0.05) in the treatment group than in the control group at various time points. Moreover, the treatment group had lower serum cortisol (Cor) and noradrenalin (NA) levels and higher levels of free triiodothyronine (FT3), free thyroxine (FT4) and thyroid-stimulating hormone (TSH) than those of (p < 0.05).
Conclusion: Insulin pump infusion effectively relieves the comprehensive stress state of patients suffering from DKA, and its therapeutic effect is superior to that of continuous instillation of low-dose insulin.
Introduction
Diabetic ketoacidosis (DKA) refers to pathological changes, such as hyperglycaemia, hyperketonaemia, electrolyte disturbance, metabolic acidosis and ketonuria, as a result of insulin insufficiency under the effects of acute infection, improper treatment or metabolic disturbances induced by a diet failing to control diabetes [1,2]. Insulin insufficiency is the leading cause of DKA. Thus, the key to treating DKA is to correct the acidosis and hyperketonaemia induced by acute metabolic disturbance by providing low-dose insulin [3,4].
The conventional therapy for DKA is continuous intravenous injection of low-dose insulin, but it is associated with complications, such as a slow recovery of blood glucose levels, a high risk of hypoglycaemia, and slow negative conversion of ketone bodies [5]. Insulin instilled intravenously at a concentration of 20 % was found to be absorbed by the wall of the infusion tube; thus, the curative effect of insulin administered via this method is decreased by absorption [6]. Currently, an insulin pump is considered an effective treatment for DKA [7,8]. Such a system consists of a pump, small injector and infusion tube that continuously infuses insulin beneath the skin of patients to maintain a stable blood glucose level by simulating pancreatic secretion. Consequently, patients absorb insulin continuously, thereby maintaining a highly stable blood insulin concentration. Moreover, the primary dose prior to eating can be adjusted according to disease conditions and blood glucose levels. Using an insulin pump, blood glucose is maintained at a normal level, and glycosylated haemoglobin (HbAlc) and the incidence of hypoglycaemia are reduced significantly [9,10].
In a DKA state, acute hyperglycaemia and fluctuations in blood glucose levels can result in the changes in oxidative stress and stress hormone levels [11]. This study explored the effects of insulin pump treatment on the comprehensive state of patients suffering from DKA.
Methods
Subjects
A total of 240 patients who were suffering from DKA who received treatment at the First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, China between February 2011 and February 2014 were selected as research subjects. The study was approved by the Medical Ethics Committee of The First Affiliated Hospital of Zhengzhou University (approval number: JWJ20150627), and conformed to the principles of the Declaration of Helsinki [12]. Patients aged 35–65 years who met the diagnostic criteria for DKA and had a blood glucose level > 13.9 mmol/L, blood pH < 7.35, ketonuria positivity, anion gap (AG) > 16 mmol/L and HCO3 level < 18 mmol/L were included. Patients with DKA induced by acute cardiovascular and cerebrovascular diseases, gastrointestinal haemorrhage, major surgery or pregnancy were excluded. Patients (N = 240) were divided randomly into treatment and control groups using a random number table.
Methods
Patients in the two groups were administered supportive treatment, such as fluid infusion, acid-base imbalance correction and electrolyte disturbance correction, upon admission to the hospital. Patients in the control group were treated with intravenous instillation of low-dose insulin (4–6 U/h), whereas patients in the treatment group were treated with intravenous insulin administered by an insulin pump at a rate of 4–6 U/h. The peripheral blood glucose level was measured before eating, 2 h after eating, and before bedtime. The dose of insulin was adjusted according to disease condition.
Observation indices
Blood gas analysis, measuring carbon dioxide combining power (CO2-CP) and AG levels, was performed in all patients at admission and 2 h and 24 h after treatment. Elbow venous blood (5 mL) was drawn from each patient at different time points. The blood samples were centrifuged, and the supernatant was used for determination of levels of HbAlc, fasting blood glucose (FBG)) and C-reactive peptide and oxidative stress-associated indices, including superoxide dismutase (SOD), malondialdehyde (MDA), glutathione peroxidase (GSH-PX) and the total antioxidant capacity (TAC), as well as levels of stress-associated hormones, including cortisol (Cor), noradrenalin (NA), free triiodothyronine (FT3), free thyroxine (FT4) and thyroid-stimulating hormone (TSH).
The FBG level was measured using a fully automatic biochemical analyser. The HbAlc level was measured using high-performance liquid chromatography. Levels of C-reactive peptide, Cor, SOD, MDA, GSH-PX and TAC were measured using chemiluminescence methods. Levels of the other hormones were measured using enzyme linked immunosorbent assay (ELISA).
Statistical analysis
Data were analysed using SPSS software (ver. 19.0) and expressed as mean ± SD. Comparisons between groups were performed using independent-sample t-tests. Enumerated data were compared using χ2 tests. Differences were considered statistically significant when p < 0.05.
Results
General data
The control group consisted of 64 males and 56 females, with an average age of 52.63 ± 7.21 years, body mass index (BMI) of 23.92 ± 2.03 kg/m2 and duration of diabetes of 7.65 ± 2.13 years. There were 62 cases of hypertension and 34 of coronary heart disease. The treatment group consisted of 66 males and 54 females, with an average age of 53.14 ± 7.28 years, BMI of 24.03 ± 2.12 kg/m2 and duration of diabetes of 7.87 ± 2.08 years. There were 66 cases of hypertension and 36 of coronary heart disease. Differences in sex, age, BMI and duration of diabetes between the two groups were not statistically significant; thus, the results were comparable.
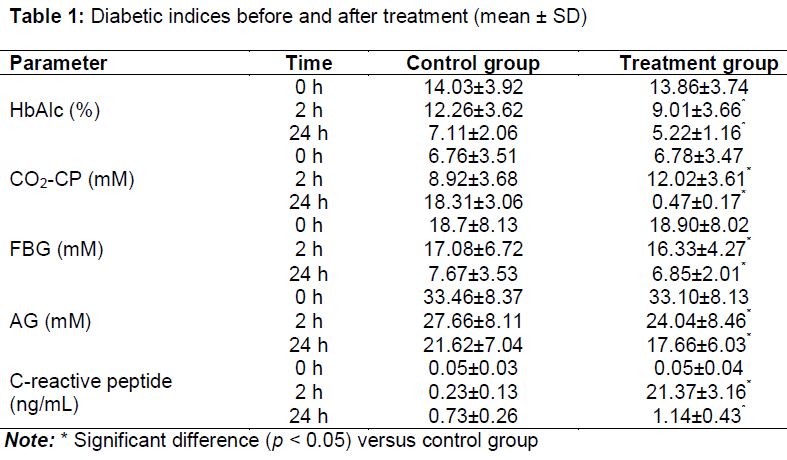
Diabetic indices before and after treatment
No significant differences were observed in any of the indices between the two groups (p > 0.05). Levels of HbAlc, FBG and AG were much lower, and the CO2-CP and C-reactive peptide levels higher, in the treatment group than the control group 2 h and 24 h after treatment ().
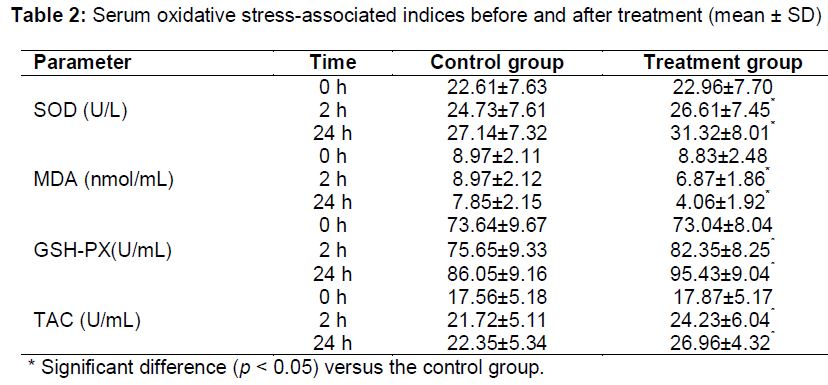
Serum oxidative stress-associated indices
Levels of SOD, GSH-PX and TAC showed no significant differences between the two groups before treatment (p > 0.05). At 2 h and 24 h after treatment, the serum MDA level was much lower, and SOD, GSH-PX and TAC levels much higher, in the treatment group than the control group (p < 0.05; ).
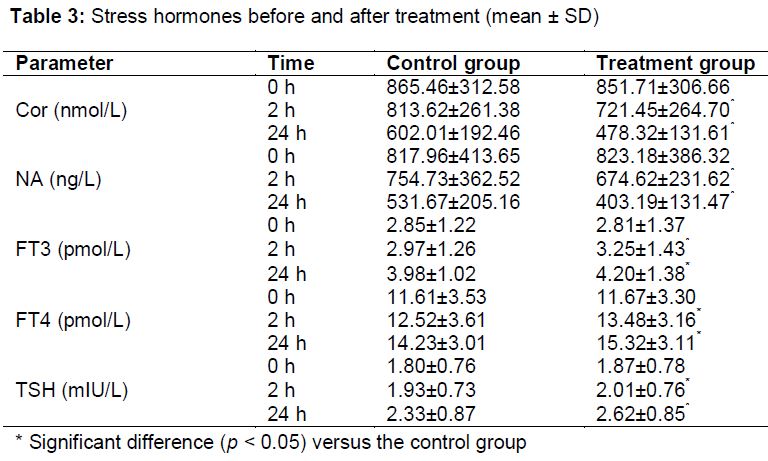
Stress hormone levels before and after treatment
Differences in levels of serum Cor, NA, FT3, FT4 and TSH between the two groups were not statistically significant before treatment (p > 0.05). Levels of serum Cor and NA were much lower, whereas the levels of FT3, FT4 and TSH were much higher, in the treatment group than the control group (p < 0.05) 2 h and 24 h after treatment ().
Discussion
DKA is a complication commonly observed in patients suffering from diabetes. Epidemiological investigations suggest that the incidence of DKA is between 15 and 45 %. DKA occurs when severe insulin insufficiency significantly weakens biological functions, such as cell differentiation and glucose utilisation, thereby increasing blood glucose levels. This resulting energy insufficiency accelerates cell differentiation and increases blood and urinary ketone levels, ultimately inducing the clinical symptoms and signs of metabolic acidosis [13,14]. Thus, the key to treating DKA is rapid control of the disease condition, and insulin treatment is absolutely necessary [15]. Low-dose insulin has great significance in the treatment of DKA. One study [16] suggested that early application of insulin effectively controlled acute onset of DKA by decreasing blood glucose levels, regulating the amplification cascade of inflammatory factors and relieving the stress state. Infusion of insulin using a insulin pump can help maintain stable blood insulin levels by controlling the infusion rate. Compared with conventional intravenous instillation of insulin, it can lower the level of blood glucose level more gradually and prevent hypoglycaemia [17].
In this study, the comprehensive stress state of patients with DKA was evaluated before and after micropump treatment, and the curative effect of the micropump was compared with that of intravenous instillation of low-dose insulin. The results demonstrated that the levels of HbAlc, FBG, and AG were significantly lower, and the levels of CO2-CP and C-reactive peptide much higher, in the treatment group than the control group, suggesting that insulin pump treatment induced a more rapid and stronger curative effect.
Patients with DKA demonstrate oxidative damage and high stress hormone levels. It has been found that the high expression of proinflammatory factors in patients with DKA can induce synthesis of acute-phase proteins, proliferation and differentiation of T cells, mass synthesis of reactive oxygen intermediates, leading to lipid peroxidation, and stress reactions [18]. Activation of the hypothalamus-pituitary-adrenal gland, gonads, thyroid gland axis, and sympathetic nervous system are also involved in the common stress reaction observed in DKA. Under DKA conditions, the body produces stress hormones such as epinephrine, noradrenalin and glucocorticoids to initiate stress defence mechanisms and induce systemic inflammatory reaction syndrome, which can ultimately lead to multiple organ failure [19-22]. In the present study, the improvements in oxidative stress and stress hormones observed in the treatment group were more obvious than those in the control group, suggesting that oxidative damage and stress were effectively controlled. Thus, the value and curative effect of an insulin micropump system in the treatment of DKA were confirmed.
Limitations of the study
Insulin pump treatment is not applicable to patients with severe DKA because of their poor insulin absorption which arises from circulatory failure. Thus, patients with severe DKA were not included in this study. The therapeutic effect of insulin pump in treating severe DKA needs further investigation.
Conclusion
Patients treated with insulin pump show more obvious changes in their comprehensive stress state, compared with those treated with intravenous instillation of low-dose insulin. Insulin pump treatment improves DKA-associated indices. Thus, insulin pump treatment, which can more effectively relieve the stress state and lower blood glucose levels of patients, needs further studies before it can be promoted for clinical application.
Declarations
Acknowledgement
References
Archives


News Updates